.webp)


Intensive Outpatient Treatment Paola: Flexible Care
Key Takeaways
- Intensive outpatient programs in the Paola area deliver at least nine clinical hours weekly through evening or early-morning blocks, letting working adults keep jobs and family routines intact 6.
- Pooled research rates IOP evidence as high, with substance use outcomes comparable to inpatient or residential care for many adults — though program quality varies significantly 2.
- Federal protections under 42 CFR Part 2 and HIPAA block employer disclosure without written consent, and FMLA certification can secure schedule flexibility without naming a diagnosis 5.
- Before committing, verify KDADS licensing, confirm a treatment plan within seven days of admission, review specific weekly schedule blocks, and request a written benefits estimate 3, 10.
When recovery has to fit around a job in Miami County
You already know what's at stake. You have a job that needs you on Monday morning, kids who need pickup at 5:15, and a calendar that doesn't have a 30-day blank space in it. You also know something has to change. That tension — the one between getting real treatment and not blowing up the life you've built — is exactly what intensive outpatient care was designed to hold.
Here's the honest version: yes, fitting structured treatment around a 9-to-5 in Paola is hard. It's also doable, and people in Miami County and the wider Kansas City metro do it every week. An intensive outpatient program (IOP) typically runs nine or more hours a week of group, individual, and medication-related care, scheduled in evening or early-morning blocks so your work hours stay mostly intact 6.
This guide is written for you as a working adult, not as a beginner. You'll get a clear map of what a credible IOP looks like in Kansas, how the schedule actually works around a commute, what privacy protections cover you, and how to tell whether the program you're considering is the real thing.
What an intensive outpatient program actually is
The 9-hour weekly floor and what it covers
Strip away the brochure language and an intensive outpatient program is built on a simple structural floor: at least nine hours of clinical time per week, delivered across multiple days, for people who don't need 24-hour supervision but need more than a once-a-week therapy hour 2. That nine-hour figure isn't a marketing number. It's the threshold federal payers like Medicare use to define what counts as IOP in the first place 6.
What fills those hours tends to look similar from program to program, even if the branding varies. You'll see group therapy as the backbone — usually two to three group sessions a week, often cognitive behavioral or relapse-prevention focused. Add an individual therapy session, family or couples sessions when relevant, and medication management with a prescriber when medication-assisted treatment is part of your plan 6.
For substance use treatment specifically, a credible IOP also includes structured assessment, an individualized treatment plan, and ongoing review of your progress against that plan 3. The pieces aren't exotic. The value is in the dose: enough clinical contact each week to actually move something, scheduled tightly enough that it can sit alongside your job rather than replace it.
Where IOP sits between higher care and weekly therapy
Picture the levels of care as a staircase, not a menu. At the top sits medical detox and residential or inpatient treatment, where you're on-site around the clock. A step down is partial hospitalization, which still asks for most of your daytime hours. IOP sits below that — structured and clinically serious, but designed to leave evenings, mornings, or both free depending on the schedule 6.
Below IOP is standard outpatient: a weekly therapy session, maybe a monthly check-in with a prescriber. That's maintenance, not active stabilization.
For someone managing a career, IOP is usually the bridge in one of two directions. You might be stepping down from residential or PHP and need a structured handoff so the gains you made don't quietly erode once you're back at your desk. Or you might be stepping up from weekly therapy because the situation has outgrown that container, and you need more clinical contact without leaving your job. Either way, IOP is the level designed for people whose recovery has to coexist with the rest of their life.
The evidence: IOP can match residential outcomes
Here's the part that probably matters most to you: does outpatient care actually work, or is it the lighter option people settle for when they can't take a month off?
The strongest answer in the peer-reviewed literature comes from a Psychiatric Services review that pooled 12 studies and one earlier review of intensive outpatient programs published between 1995 and 2012. The reviewers rated the evidence base as high. Across randomized trials and naturalistic analyses of adults in substance use treatment, IOP produced reductions in alcohol and drug use that were equivalent to those seen in inpatient or residential care 2. Same direction, comparable magnitude — for the population studied.
That's a real finding, and it deserves to be stated carefully. The review looked at adults in substance use disorder treatment, defined IOP as nine or more hours of clinical contact per week, and covered programs studied over a roughly 17-year window. The authors also flagged something honest: programs varied a lot in how they were actually run, which makes it harder to say every IOP performs identically 2. The headline isn't "outpatient equals inpatient in every situation." The headline is that for many adults working on a substance use disorder, a well-structured outpatient program can get you to the same place a bed-based program would — without asking you to disappear from your life for 30 days.
For someone weighing whether to keep working while you do this, that's a meaningful piece of news. You're not choosing a watered-down version of treatment. You're choosing a different delivery model for clinical care that the evidence supports as a legitimate path. The catch is that "well-structured" matters. Programs vary, which is why how you vet the one you pick — staffing, hours, treatment planning, what happens when you struggle — ends up doing a lot of the work the brochure can't.
What a real week looks like around a 9-to-5
Here's the part most pages skip. You don't need a philosophy of recovery — you need to know what Tuesday looks like.
A typical IOP week is built around three evening group sessions, usually somewhere in the 5:30 to 8:30 window, plus one individual therapy hour and a medication-management check-in when that applies. Stack those together and you're at the nine-plus clinical hours per week that defines IOP in the first place 2. Some programs add a Saturday morning option for people whose evenings are non-negotiable because of a partner's shift or a kid's practice schedule.
Run that against a normal week. You leave the office at 5, drive home or to the program, eat something, and you're in group by 5:30 or 6. You're home by 9. You've kept your work hours. You've kept dinner most nights. You've also done real clinical work — the kind that involves a curriculum, a therapist who knows your name, and a group of people who will notice if you ghost on Thursday.
The morning option matters more than it sounds. If your job has hard evening commitments — a recurring client call, coaching at the school, a partner who travels — a 7 a.m. group before work can replace one of the evening blocks. You sit with coffee, do the session, and you're at your desk by 9 or 9:30 6.
Most programs run somewhere between 8 and 16 weeks at this intensity, then taper. That's the realistic horizon to plan around when you talk to a manager about a slightly modified schedule, or when you map out childcare. It's a season of your life, not a permanent rearrangement of it.
Will some weeks feel like a lot? Yes. Driving to a 6 p.m. group after a hard day at work is its own small act of follow-through. The reward is that on Friday you've done something — not waited for a future window that never opens.
Privacy, your employer, and what people actually see
Confidentiality protections that apply to IOP records
Your treatment records are not your employer's business, and federal law treats them that way. Substance use treatment records held by a licensed program are protected by 42 CFR Part 2, a federal rule that's stricter than standard HIPAA. In plain terms: a Kansas-licensed IOP can't confirm you're a patient, share your attendance, or release any clinical information without your specific written consent for each disclosure. No casual phone call from a curious manager will get past the front desk.
Mental health records held by the same program fall under HIPAA, which also blocks disclosure to your employer absent your written authorization. Programs operating under KDADS licensing in Kansas are bound by both layers depending on what's being treated 5, 3.
FMLA, scheduling, and what HR is and isn't told
Here's the part that surprises people in a good way: most working professionals in IOP never tell HR anything specific. Evening and early-morning groups exist precisely so you don't have to. If your sessions are at 6 p.m. on Monday, Wednesday, and Thursday, you simply leave at 5 like everyone else 6.
If you do need schedule flexibility — say a 7 a.m. group means a 9:30 arrival twice a week — you have options. The Family and Medical Leave Act allows eligible employees at covered employers to take job-protected leave, including intermittent leave, for a serious health condition. Substance use disorder treatment by a healthcare provider qualifies. You give HR a medical certification form, which states you need leave for treatment of a serious health condition. It does not name your diagnosis, your provider, or what kind of treatment you're receiving.
You can also frame it as ongoing medical appointments without invoking FMLA at all. The detail you share is your decision, not theirs to demand. That distinction is worth holding onto.
How Kansas regulates the program you're considering
Kansas doesn't leave outpatient substance use treatment to the honor system. Any program calling itself an IOP in this state has to be licensed by the Kansas Department for Aging and Disability Services (KDADS), the agency that sets the rules for behavioral health facilities and the SUD treatment levels that sit underneath them 5, 3.
What that licensing actually buys you matters. KDADS-licensed programs have to do an individualized treatment plan within seven days of admission, follow staffing ratios, and document your progress against measurable goals — not just count attendance 10. If a program can't tell you when your treatment plan will be written or who is signing off on it, that's a flag worth taking seriously.
The funding side has been moving in your favor. Under the KanCare 1115 demonstration, Kansas expanded access to the full SUD continuum using ASAM-based placement criteria, which is the standard clinical framework for matching people to the right level of care. The waiver also opened the door wider for telehealth, which matters if your commute pulls you between Paola and the Kansas City metro on different days of the week 7. In April 2025, the state went further and approved a Medicaid amendment adding PHP and IOP coverage for mental health conditions tied to eating disorders — evidence that Kansas is actively building out, not pulling back from, this level of care 1, 4.
When you call a program, ask directly: Are you KDADS-licensed for outpatient SUD services? Who writes my treatment plan, and when? Those two answers tell you most of what you need to know.
When mental health challenges and addiction intersect, it can feel isolating. At Arista, we offer compassionate, evidence-based, and trauma-informed care to help you heal, grow, and move forward.
Paola, the KC metro, and the prevalence picture
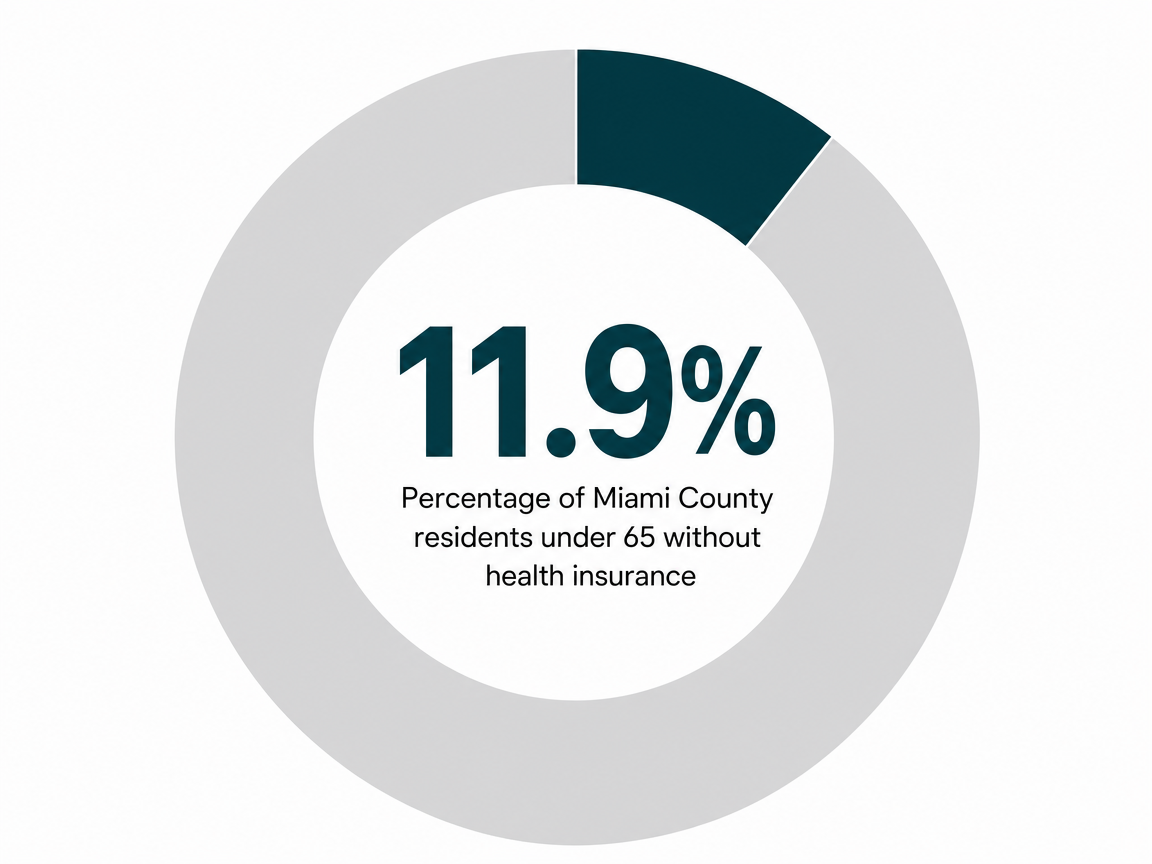
One quiet advantage of being in Paola: you're close enough to the Kansas City metro to have real options, far enough out that running into a coworker in the parking lot of an evening group is unlikely. Paola sits in Miami County with about 5,835 residents and a median household income of $73,281, and roughly 11.9% of people under 65 are uninsured — a small, stable community with the kind of highway access that makes a 30- or 40-minute drive to a program in the southern metro a normal commute, not a logistical event 12.
That geography matters more than it sounds. You can choose a program in town for convenience, or pick one across the county line for a layer of separation from your professional circle. Both are valid. Neither is uncommon.
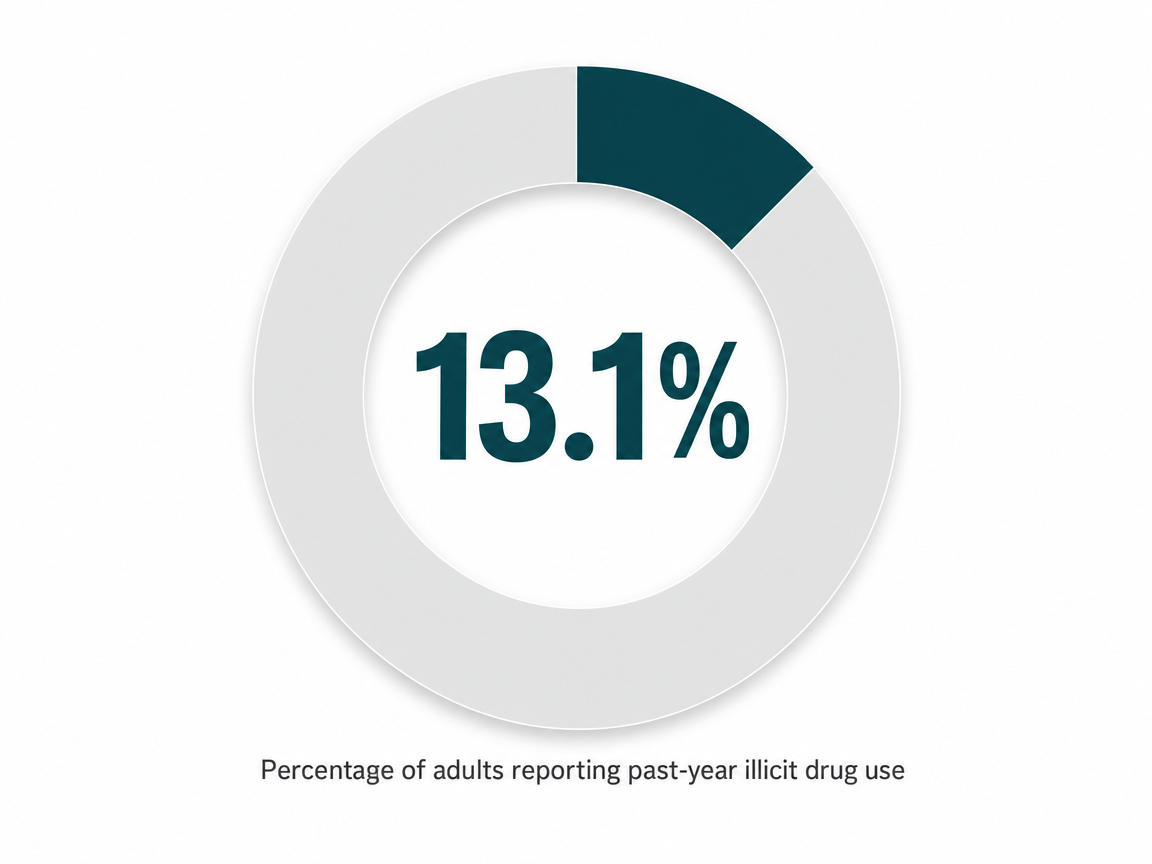
The need in this region is real, and worth seeing in plain numbers. SAMHSA's National Survey on Drug Use and Health, looking at adults 12 and older across the Kansas City metropolitan statistical area between 2005 and 2010, found:
- 13.1% reported past-year illicit drug use
- 8.6% met criteria for a substance use disorder
- 6.5% had experienced a major depressive episode in the past year 8
Those rates tracked closely with Missouri and U.S. averages — Paola-area residents aren't outliers, and you aren't either.
What that means in practical terms: there is established demand, established licensed capacity, and you are not the first professional in this corner of Kansas to make this call.
Paying for it: insurance categories without the guesswork
Money is usually the second question after privacy, and it deserves a straight answer. The good news is that intensive outpatient care, when delivered by a licensed program, falls into recognized billing categories across all three major payer types you're likely to be working with.
If you have commercial insurance through your employer, IOP for substance use and mental health is generally a covered behavioral health benefit. Your plan documents will list it under outpatient mental health or substance use treatment, often with a per-session copay or a coinsurance share after your deductible. Ask the program's intake team to run a benefits verification before your first session — they do this every day, and it gives you a written estimate of what you'll owe per week.
If you're on KanCare, Kansas Medicaid covers IOP as part of the SUD continuum that the state expanded under its 1115 demonstration, with ASAM-based placement determining the right level for you 7. As of April 2025, Kansas also added Medicaid coverage for IOP tied to mental health conditions related to eating disorders, a sign the state is widening rather than tightening this benefit 1, 4.
If you qualify for Medicare Part B, IOP is covered when delivered by an approved facility and meets the nine-hours-a-week clinical threshold 6.
The point isn't to memorize codes. It's to know that the program you call should be able to verify your benefits, give you a written cost estimate, and tell you what your weekly out-of-pocket looks like before you commit. If they can't, that's information too.
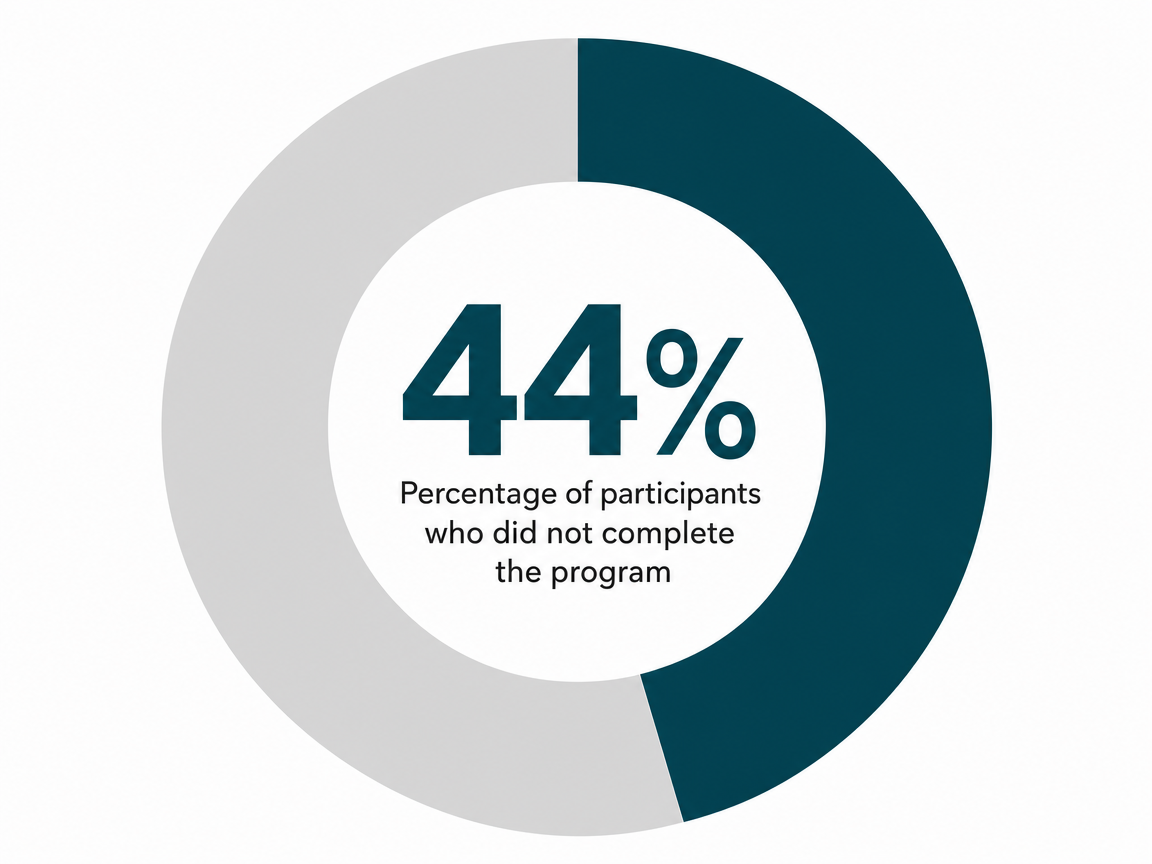
What completers say works — and the dropout no one mentions
When researchers asked 65 people who finished a four-month integrated IOP what actually helped, the answers were less clinical than you might expect. Mean satisfaction landed at 9.35 out of 10 for clinic time and 9.17 for the program overall. The themes that kept surfacing weren't curriculum names or therapy modalities. They were relationships with peers in the group, the warmth of the staff, and a sense of self-development that built week over week 11.
Hold onto that. The thing that gets people through is not a worksheet. It's the Tuesday night room where someone remembers what you said last week and asks how it went.
Signals you're ready to step down (or step into) IOP
How do you know it's time? The honest answer is that the signals look different depending on which direction you're moving from.
If you're stepping down from residential or partial hospitalization, the green lights tend to cluster: you've completed detox if it was needed, your cravings are manageable without round-the-clock support, you have a place to sleep that doesn't actively pull you backward, and your treatment team agrees that ASAM-based placement criteria point to a less intensive level of care 7. Stepping down isn't a graduation. It's a handoff, and IOP is built to catch you.
If you're stepping up from weekly therapy, the signals are quieter and easier to miss. You're keeping appointments but not really moving. You've had a slip, or several. The hour a week isn't holding the weight anymore. That's not a failure of your therapist or of you — it's information that the container needs to get bigger for a while.
Either way, a licensed program will run a clinical assessment before placing you, not after 3. Trust that process. You don't have to diagnose yourself before you call.
How to vet a Paola-area program in one phone call
You don't need a clinical background to size up a program. You need about fifteen minutes on the phone and the right five questions.
- Start with licensing. Ask if the program is licensed by KDADS for outpatient substance use disorder services, and have them say it plainly 5, 3. A real intake coordinator will not hesitate.
- Ask about the treatment plan. Who writes yours, when does it get written, and how often is it reviewed? Kansas-licensed programs are expected to have an individualized plan in place within seven days of admission 10. If the answer is vague or sounds like a template, keep calling.
- Ask what the schedule actually looks like. You want to hear specific evening and morning blocks that add up to nine or more hours a week, not a sales pitch 2, 6.
- Ask what happens if you miss a session — does someone reach out, or do you just disappear from the roster? That answer tells you whether the program treats attendance as a relationship or a checkbox.
- Ask them to verify your benefits before your first session and put the weekly cost estimate in writing. Commercial, KanCare, or Medicare Part B — they should handle this without flinching.
If you'd rather not start with a clinic at all, the SAMHSA National Helpline at 1-800-662-HELP offers free, confidential referrals around the clock 9. One call. That's the whole first step.
Frequently Asked Questions
How many hours a week does intensive outpatient treatment in Paola actually require?
Plan on at least nine hours of clinical time per week. That's the threshold federal payers use to define IOP, and it's typically delivered as three group sessions plus an individual hour and medication management when relevant 6. Most programs run those hours in evening blocks, with some offering an early-morning option so you can keep your work hours largely intact.
Will my employer find out I'm in an IOP?
Not unless you tell them. Substance use treatment records at a licensed program are protected by 42 CFR Part 2, and mental health records by HIPAA — neither allows disclosure to your employer without your written consent 5. Evening and early-morning groups exist precisely so you don't need a schedule conversation. If you do want flexibility, FMLA medical certification names a serious health condition without naming your diagnosis.
Is intensive outpatient treatment really as effective as going to inpatient or residential care?
For many adults working on a substance use disorder, yes. A Psychiatric Services review of 12 studies plus one earlier review (1995–2012) rated the IOP evidence base as high and found reductions in alcohol and drug use comparable to inpatient or residential care 2. The authors noted programs vary in how they're run, so vetting the specific program matters more than the level-of-care label on the door.
Does KanCare or my commercial insurance cover IOP in Kansas?
Generally yes for both. KanCare covers IOP as part of the SUD continuum expanded under the state's 1115 demonstration, with ASAM-based placement determining your level 7. Kansas added Medicaid IOP coverage for eating-disorder-related mental health in April 2025, a sign the benefit is widening 1. Commercial plans typically cover IOP under outpatient behavioral health benefits — ask intake to verify and put weekly costs in writing.
How do I know if I'm ready to step down from a higher level of care into IOP?
You don't have to decide alone. A licensed program will run a clinical assessment using ASAM placement criteria before placing you 7. The signals tend to cluster: detox is complete if it was needed, cravings are manageable without round-the-clock support, you have a stable place to sleep, and your treatment team agrees a less intensive level fits. Stepping down is a handoff, not a graduation.
What should I ask a Paola-area program before I commit?
Five questions cover most of it. Are you KDADS-licensed for outpatient SUD services 3? Who writes my treatment plan, and will it be done within seven days 10? What does the weekly schedule look like in real evening and morning blocks 2? What happens if I miss a session — does someone reach out? Can you verify my benefits and give me a written weekly cost estimate?
References
- KS-25-0005 - Medicaid. https://www.medicaid.gov/medicaid-spa/2025-04-17/178831
- Substance Abuse Intensive Outpatient Programs: Assessing the Evidence. https://pmc.ncbi.nlm.nih.gov/articles/PMC4152944/
- Substance Use Disorder Treatment Services - KDADS. https://www.kdads.ks.gov/services-programs/behavioral-health/services-and-programs/substance-use-disorder-treatment-services
- [PDF] Kansas State Plan Amendment (SPA) – KS-25-0005 - Medicaid. https://www.medicaid.gov/medicaid/spa/downloads/KS-25-0005.pdf
- Behavioral Health Licensing | Department for Aging and Disability Services - KDADS. https://www.kdads.ks.gov/licensing-policy/behavioral-health-licensing
- Mental health care (intensive outpatient program services) - Medicare. https://www.medicare.gov/coverage/mental-health-care-intensive-outpatient-program-services
- KS DSRIP Evaluation Design Approval Letter.pdf. https://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Waivers/1115/downloads/ks/ks-kancare-ca.pdf
- Substance Use and Mental Disorders in the Kansas City MSA. https://www.samhsa.gov/data/sites/default/files/NSDUHMetroBriefReports/NSDUHMetroBriefReports/NSDUH-Metro-Kansas-City.pdf
- National Helpline for Mental Health, Drug, Alcohol Issues - SAMHSA. https://www.samhsa.gov/find-help/helplines/national-helpline
- State Residential Treatment for Behavioral Health Conditions: Kansas Summary. https://aspe.hhs.gov/sites/default/files/2021-08/StateBHCond-Kansas.pdf
- Clients' Experiences and Satisfaction with an Integrated Intensive Outpatient Program. https://pmc.ncbi.nlm.nih.gov/articles/PMC11898248/
- U.S. Census Bureau QuickFacts: Paola city, Kansas. https://www.census.gov/quickfacts/fact/table/paolacitykansas/PST045224
You’re not alone in this.
When mental health challenges and addiction intersect, it can feel isolating. At Arista, we offer compassionate, evidence-based, and trauma-informed care to help you heal, grow, and move forward.
Support that moves with you.
You’ve taken a brave first step. At Arista Recovery, we’re here to help you continue with best-in-class care designed for long-term healing and support.





